
Pros and Cons of SRS methods
This is not going to be a usual article with an intro, body and conclusions. It is just a list of advantages and disadvantages of some of the different methods of Sex Reassignment Surgery (SRS methods) in Male to Female Transsexuals.
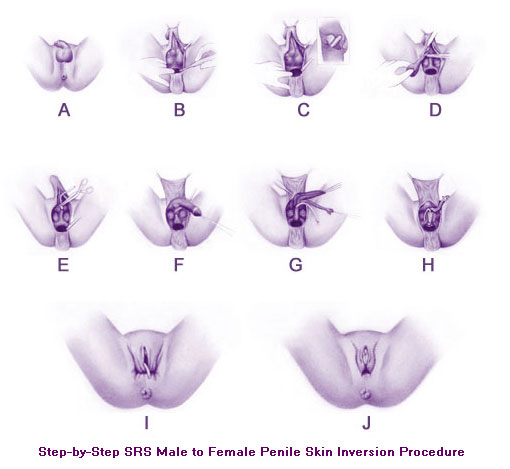
PENILE INVERSION VAGINOPLASTY
Pros
- Method of first choice for most surgeons and Subjects
- Less Invasive, faster recovery time.
- Less Chance of post operative complication
- Neo Vagina has nerve endings and thus has sensation.
- Usually cheaper
Cons
- Depth depends on available skin and surgeon’s skills
- Needs to be dilated, daily in the beginning. Or the Vagina will shrink or even collapse totally
- Dry. The tissue inside the vagina does not produce mucus. You have to lubricate it during sex
- Possibility of hair inside the vagina
- the vagina reportedly feels a little different to the sexual partner
- Skin used for the vaginal lining is thin an there is a possibility of it’s being ruptured.
SIGMOID COLON VAGINOPLASTY
Pros
- Self Lubricating
- Tissue used in the vaginal lining produces mucus, just like the vigina in cis-females. Reportedly feels like the same to a sexual partner.
- Thicker tissue, less chance of rupturing.
- No possibility of hair inside the vagina
- (No doctor told me this, just speculation on my part) Since the penile and scrotal skin are not used for creating the vagina, more skin is available to create the labia majora, labia minora, clitoral hood etc. Thus a more aesthetically pleasing vulva can be created.
- The vagina has it’s own blood supply (since it was part of the digestive tract). Thus there is less chance of atrophy/collapse.
Cons
- More Invasive, more chance of post operative complication, longer recovery time.
- Less number of surgeons trained in this method.
- No sensation inside the vagina
- The supposedly self lubricating mucus lining can flow heavily and you will have to wear sanitary pads or tampons. And it is not like menses in the sense that the colon is a piece of the elementary canal and smells really bad. This issue reportedly resolves itself for most girls in about a year but I have heard of cases where it was so bad and protracted that the subject was considering sealing off the new vagina.
- The elementary canal is cut, a piece (the rising part of the sigmoid colon usually) re positioned to form the vagina and the digestive canal sewn back together. Than the elementary canal needs to STOPPED for about a week. These are all rife with potential for complication.
- A huge scar on the lower abdomen, transverse/horizontal, about 20 Centimeters in length.
- Possible weakening of the lower abdominal muscles and hence a bulge in the lower belly after recovering from the surgery. This happens because the doctors have to cut through the muscles to get to the abdominal cavity.
I am sure there are more Pros and cons for both methods that I cannot recall right now at the spur of the moment. I will update them as as I remember. If you know of any that I have missed, please do us the favor of leaving a comment or dropping us a mail.
About which method to choose, I can only repeat one doctor told me. Sigmoid Colon Vaginoplasty is Conceptually Elegant but not Very Practical. It could be used for a revision vaginoplasty if things do not work out well or there is a compelling reason like the patient having undergone removal of both penis and scrotum (as happens in some Trans Communities). But it should not be the first resort. Even in cases where the available skin is not enough, a Penile Inversion with Skin Graft can be carried out.
Now for a couple of disclaimers and notes:
- I am not a doctor and this should not be construed as medical advice. It is just some of the things I learned when I was doing research for my own surgery and decided to pass along.
- This two methods are not the only methods. One very obvious one that I have left out is the SINGAPORE FLAP. A strip of skin from either side of the line between the abdomen and legs is harvested and used to make a vaginal canal.
- Doctors are evolving surgical methods all the time. Dr. Supron had pioneered some of the current methods. I exchanged a few e-mails with Dr. Chet in Thailand. He uses a method that cannot be clubbed into either of the 3 I have mentioned. Again there are doctors who harvest some of the glands in the area and use it produce some modicum of lubrication in the vagina.
2 Comments
Can u give a brief information of all the techniques you mentioned in disclaimer and notes
Just a comment on sigmoid. The incision made to do the colon portion of the surgery is very small in most cases and is done on a second surgical visit. It is usually split up into two visits.